Blank Fa 29 Nevada PDF Template
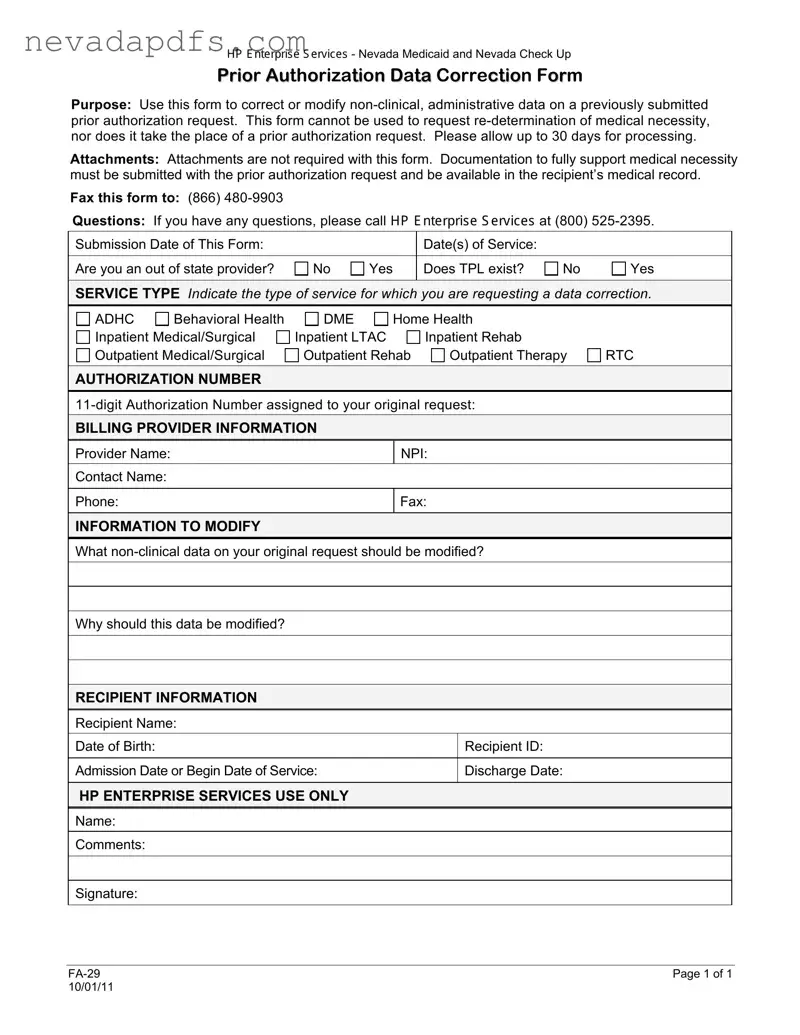
The FA 29 Nevada form serves a crucial role in the administration of Nevada Medicaid and Nevada Check Up by allowing providers to correct or modify non-clinical, administrative data on previously submitted prior authorization requests. It is essential to understand that this form is not intended for requesting a re-determination of medical necessity, nor does it replace the original prior authorization request. Providers must be aware that processing this form may take up to 30 days. While attachments are not required, it is imperative that all documentation supporting medical necessity is submitted with the initial prior authorization request and remains accessible in the recipient’s medical record. The form includes sections for essential information such as service type, authorization number, and recipient details, ensuring that all necessary modifications are clearly communicated. Providers are also required to indicate whether they are out-of-state and if third-party liability exists. The form must be faxed to the designated number, and any questions can be directed to the provided contact number. Timely and accurate completion of the FA 29 form is vital for maintaining compliance and ensuring that recipients receive the necessary services without undue delay.
Fa 29 Nevada Sample
+3 ( QWHUSU VH 6 HUY FHV - Nevada Medicaid and Nevada Check Up
PRIOR AUTHORIZATION DATA CORRECTION FORM
Purpose: Use this form to correct or modify
Attachments: Attachments are not required with this form. Documentation to fully support medical necessity must be submitted with the prior authorization request and be available in the recipient’s medical record.
Fax this form to: (866)
Questions: If you have any questions, please call +3 ( QWHUSU VH 6 HUY FHV at (800)
Submission Date of This Form: |
|
|
Date(s) of Service: |
|
|
|
|
|
|
|
|
Are you an out of state provider? |
No |
Yes |
Does TPL exist? |
No |
Yes |
|
|
|
|
|
|
SERVICE TYPE Indicate the type of service for which you are requesting a data correction.
ADHC |
Behavioral Health |
DME |
Home Health |
|
||
Inpatient Medical/Surgical |
Inpatient LTAC |
Inpatient Rehab |
|
|||
Outpatient Medical/Surgical |
Outpatient Rehab |
Outpatient Therapy |
RTC |
|||
AUTHORIZATION NUMBER |
|
|
|
|
|
|
|
||||||
BILLING PROVIDER INFORMATION |
|
|
|
|
||
Provider Name: |
|
|
NPI: |
|
|
|
Contact Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone: |
|
|
Fax: |
|
|
|
|
|
|
|
|
|
|
INFORMATION TO MODIFY |
|
|
|
|
|
|
What |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Why should this data be modified? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RECIPIENT INFORMATION |
|
|
|
|
|
|
Recipient Name: |
|
|
|
|
|
|
Date of Birth: |
|
|
|
|
Recipient ID: |
|
|
|
|
|
|
||
Admission Date or Begin Date of Service: |
|
|
Discharge Date: |
|
||
|
|
|
|
|
||
HP ENTERPRISE SERVICES USE ONLY |
|
|
|
|
||
Name:
Comments:
Signature:
Page 1 of 1 |
|
10/01/11 |
|
File Attributes
| Fact Name | Description |
|---|---|
| Purpose | This form is designed to correct or modify non-clinical, administrative data on a previously submitted prior authorization request. |
| Limitations | The FA 29 form cannot be used to request a re-determination of medical necessity and does not replace a prior authorization request. |
| Processing Time | Expect processing to take up to 30 days after submission of the form. |
| Attachments | No attachments are required with this form, but documentation supporting medical necessity must be included with the original prior authorization request. |
| Governing Law | This form is governed by Nevada Medicaid regulations and guidelines. |
Fill out Common Forms
State of Nevada Declaration of Value Form - A critical step in the real estate transfer process in Nevada.
Filing the Louisiana Articles of Incorporation form is an important first step for many entrepreneurs looking to establish a legal framework for their businesses. By providing key information such as the names of officers and the business's purpose, this document plays a pivotal role in ensuring compliance with state laws. To simplify this process, resources like UsaLawDocs.com can offer valuable guidance and support.
C4 Form Nevada - By submitting the AD-5 form, officers actively engage in a process of self-assessment, documenting career achievements and aspirations.