Blank Sr1 Nevada PDF Template
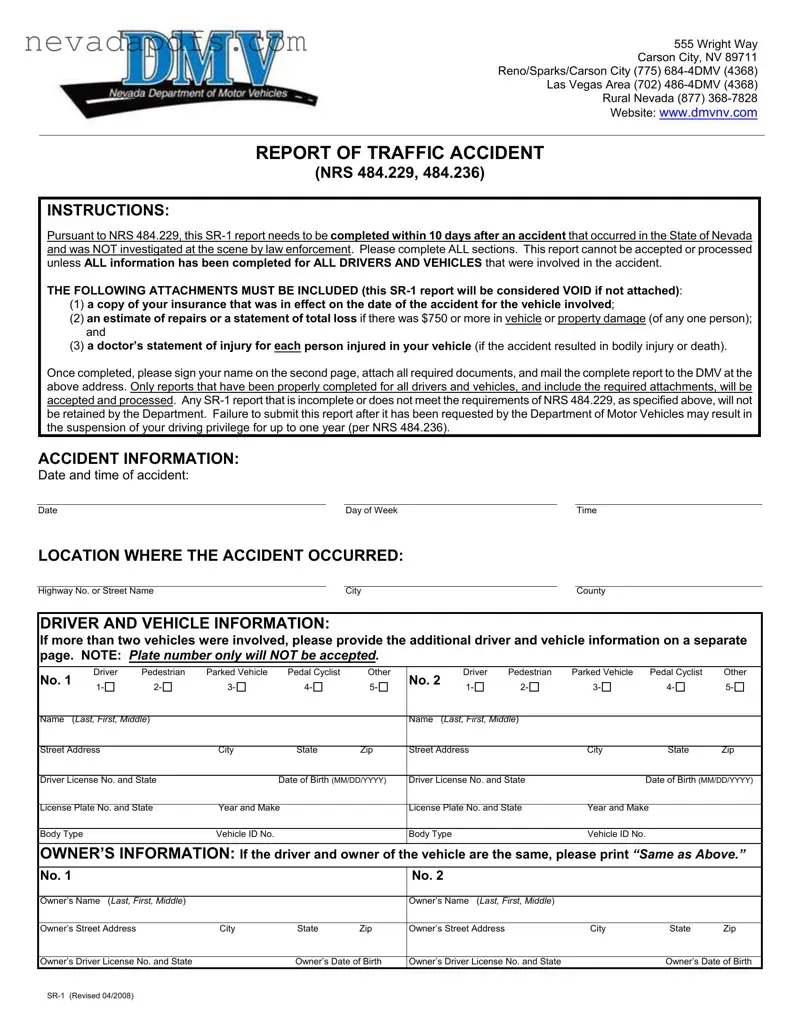
The SR-1 form is an essential document for anyone involved in a traffic accident in Nevada that was not investigated by law enforcement at the scene. It must be completed within 10 days of the incident and requires detailed information about all drivers and vehicles involved. This form serves multiple purposes, including documenting the accident and ensuring compliance with state laws. To be accepted, the SR-1 must include specific attachments: a copy of the insurance that was active at the time of the accident, an estimate of repairs or a statement of total loss if damages exceed $750, and a doctor’s statement for any injuries sustained. Failure to submit a complete report can lead to serious consequences, including the suspension of driving privileges. The form also collects crucial details such as the date, time, and location of the accident, along with personal and vehicle information for all parties involved. Understanding the requirements and ensuring all sections are filled out accurately is vital for a smooth process with the Department of Motor Vehicles.
Sr1 Nevada Sample
555 Wright Way
Carson City, NV 89711
Reno/Sparks/Carson City (775)
Las Vegas Area (702)
Rural Nevada (877)
Website: www.dmvnv.com
REPORT OF TRAFFIC ACCIDENT
(NRS 484.229, 484.236)
INSTRUCTIONS:
Pursuant to NRS 484.229, this
THE FOLLOWING ATTACHMENTS MUST BE INCLUDED (this
(1)a copy of your insurance that was in effect on the date of the accident for the vehicle involved;
(2)an estimate of repairs or a statement of total loss if there was $750 or more in vehicle or property damage (of any one person); and
(3)a doctor’s statement of injury for each person injured in your vehicle (if the accident resulted in bodily injury or death).
Once completed, please sign your name on the second page, attach all required documents, and mail the complete report to the DMV at the above address. Only reports that have been properly completed for all drivers and vehicles, and include the required attachments, will be accepted and processed. Any
ACCIDENT INFORMATION:
Date and time of accident:
DateDay of WeekTime
LOCATION WHERE THE ACCIDENT OCCURRED:
Highway No. or Street Name |
|
City |
|
County |
DRIVER AND VEHICLE INFORMATION:
If more than two vehicles were involved, please provide the additional driver and vehicle information on a separate page. NOTE: Plate number only will NOT be accepted.
No. 1 |
Driver |
Pedestrian |
Parked Vehicle |
Pedal Cyclist |
Other |
No. 2 |
Driver |
Pedestrian |
Parked Vehicle |
Pedal Cyclist |
Other |
|
1- |
2- |
3- |
4- |
5- |
1- |
2- |
3- |
4- |
5- |
|||
|
|
|||||||||||
|
|
|
|
|
|
|
|
|||||
Name (LAST, FIRST, MIDDLE) |
|
|
|
Name (LAST, FIRST, MIDDLE) |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|||
Street Address |
|
City |
State |
Zip |
Street Address |
|
City |
State |
Zip |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
Driver License No. and State |
|
Date of Birth (MM/DD/YYYY) |
Driver License No. and State |
Date of Birth (MM/DD/YYYY) |
||||||||
|
|
|
|
|
|
|
||||||
License Plate No. and State |
Year and Make |
|
License Plate No. and State |
Year and Make |
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Body Type |
|
|
Vehicle ID No. |
|
|
Body Type |
|
|
Vehicle ID No. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OWNER’S INFORMATION: If the driver and owner of the vehicle are the same, please print “Same as Above.”
No. 1 |
No. 2 |
Owner’s Name (LAST, FIRST, MIDDLE)
Owner’s Name (LAST, FIRST, MIDDLE)
Owner’s Street Address |
City |
State |
Zip |
Owner’s Street Address |
City |
State |
Zip |
Owner’s Driver License No. and State |
Owner’s Date of Birth |
Owner’s Driver License No. and State |
Owner’s Date of Birth |
INSURANCE INFORMATION:
A COPY OF YOUR INSURANCE CARD MUST BE ATTACHED TO THIS REPORT.
Please ensure to attach a copy of your insurance card that was in effect on the date of the accident for the vehicle involved. This information is necessary to verify that the vehicle was insured at the time of the accident. If insurance was not in effect on the date of the accident, your driving privilege and registration may be suspended under Chapter 485 of Nevada Revised Statutes.
ACCIDENT DESCRIPTION
Please write a brief description of the accident:
PROPERTY DAMAGE (other than the vehicle):
If you answer “Yes” below, please explain in the space provided:
Yes
No Was there damage to property other than the vehicle? If Yes, describe:
Property Owner’s Name:
Property Owner’s Address:
ESTIMATE OF REPAIRS:
AN ESTIMATE OF REPAIRS OR A STATEMENT OF TOTAL LOSS MUST BE ATTACHED if there was $750 or more in vehicle or property damage (of any one person). Pursuant to NRS 484.229, the estimate of repairs or statement of total loss must be from an established repair garage, an insurance adjuster employed by an insurer licensed to do business in the State of Nevada, an adjuster licensed pursuant to chapter 684A of NRS, or an appraiser licensed pursuant to Chapter 684B of NRS.
This
PERSONAL INJURY:
If an injury occurred, A DOCTOR’S STATEMENT OF INJURY FOR EACH INDIVIDUAL INJURED IN YOUR VEHICLE MUST BE ATTACHED. VOID if not attached!
Driver
Passenger
Name |
|
|
|
|
|
Age |
|
Sex |
|
|
|
|
|
|
|
|
|
Street Address |
|
City |
|
State |
|
Zip Code |
|
Relationship to Driver of Your Vehicle* |
|
|
|
|
|
|
|
|
*Husband, wife, son, daughter, etc. |
|
|
|
|
|
|
|
|
|
Nature and Extent of Injuries |
|
|
|
|
|
|
|
|
SIGNATURE:
By completing this report, you are authorizing the Department of Motor Vehicles to release your name, mailing address, and insurance information to the other parties involved in the traffic accident and/or to their insurer (NRS 484.229).
I hereby certify all statements made in this report are true. I agree and understand any person who completes this report knowing or having reason to believe the information is false is guilty of a gross misdemeanor. (NRS 484.236)
Signature |
Date Signed |
*** VOID IF NOT SIGNED ***
NOTE: Only reports that have been properly completed for all drivers and vehicles, and include the required attachments, will be accepted and processed. Any
File Attributes
| Fact Name | Description |
|---|---|
| Purpose of SR-1 | The SR-1 form is used to report traffic accidents in Nevada that were not investigated by law enforcement at the scene. |
| Filing Deadline | Individuals must complete and submit the SR-1 report within 10 days of the accident occurrence. |
| Required Attachments | To be valid, the report must include a copy of the insurance card, an estimate of repairs or statement of total loss, and a doctor’s statement of injury if applicable. |
| Governing Laws | The SR-1 form is governed by Nevada Revised Statutes (NRS) 484.229 and 484.236. |
| Consequences of Non-compliance | Failure to submit the SR-1 report when requested may lead to a suspension of driving privileges for up to one year. |
Fill out Common Forms
Nevada Medicaid Renewal - Includes a portion for detailing living expenses such as shelter costs and utilities, alongside any spousal income.
When preparing to transfer ownership, obtaining a reliable thorough Trailer Bill of Sale document is crucial. This form not only serves to document the sale but also protects the interests of both the buyer and seller, ensuring all necessary details are adequately covered.
How to Get a Work Permit in Nevada - Personal information including name, date of birth, and contact details are required on the form.