Blank Universal Referral Nevada PDF Template
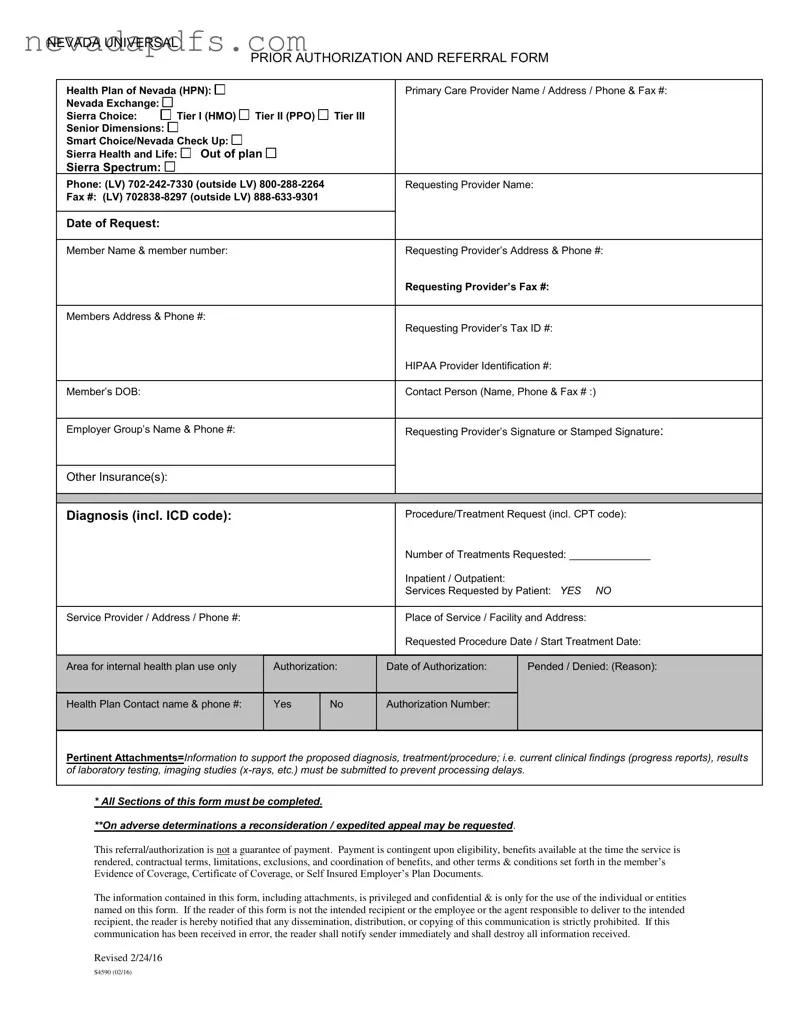
The Universal Referral Nevada form is an essential document used in the healthcare system to streamline the process of obtaining prior authorization and referrals for medical services. It is designed for use by various health plans, including Health Plan of Nevada, and covers multiple tiers such as HMO and PPO options. This form requires detailed information from both the requesting provider and the patient, including names, contact details, and medical history. Key sections of the form include the diagnosis, procedure or treatment requested, and the number of treatments needed, along with corresponding codes for accurate processing. Additionally, the form emphasizes the importance of attaching relevant clinical information to support the request, which helps prevent delays in authorization. It is crucial to note that completing all sections of the form is mandatory, as incomplete submissions can lead to processing issues. The form also contains a confidentiality notice, underscoring the importance of protecting patient information. Understanding the components and requirements of the Universal Referral Nevada form can significantly enhance the efficiency of healthcare services for patients and providers alike.
Universal Referral Nevada Sample
NEVADA UNIVERSAL
PRIOR AUTHORIZATION AND REFERRAL FORM
Health Plan of Nevada (HPN): |
|
|
|
|
|
|
|
|
|
|
|
|
Primary Care Provider Name / Address / Phone & Fax #: |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
||||||||||||||||||
Nevada Exchange: |
|
|
|
|
|
Tier I (HMO) |
|
|
Tier II (PPO) |
|
Tier III |
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
Sierra Choice: |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
||||||||||||||||
Senior Dimensions: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Smart Choice/Nevada Check Up: |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
Sierra Health and Life: |
|
|
Out of plan |
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
||||||||||||||||||
Sierra Spectrum: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Phone: (LV) |
|
|
Requesting Provider Name: |
|||||||||||||||||||||
Fax #: (LV) |
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Date of Request: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
Member Name & member number: |
|
|
|
|
|
|
|
Requesting Provider’s Address & Phone #: |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Requesting Provider’s Fax #: |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
Members Address & Phone #: |
|
|
|
|
|
|
|
Requesting Provider’s Tax ID #: |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HIPAA Provider Identification #: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Member’s DOB: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Contact Person (Name, Phone & Fax # :) |
||||||
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
Employer Group’s Name & Phone #: |
|
|
|
|
|
|
|
Requesting Provider’s Signature or Stamped Signature: |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Other Insurance(s): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
Diagnosis (incl. ICD code): |
|
|
|
|
|
|
|
Procedure/Treatment Request (incl. CPT code): |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Number of Treatments Requested: ______________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Inpatient / Outpatient: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Services Requested by Patient: YES NO |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
Service Provider / Address / Phone #: |
|
|
|
|
|
|
|
Place of Service / Facility and Address: |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Requested Procedure Date / Start Treatment Date: |
|
|
|
|
|
|
|
|
|
|||||||||||||||||
Area for internal health plan use only |
|
|
Authorization: |
|
|
|
||||||||||||||||||
|
|
Date of Authorization: |
Pended / Denied: (Reason): |
|||||||||||||||||||||
CURRENT CLINICAL FINDINGS AND |
MANAGEMENT |
|
use the space – also see requirements below and attach to this form. |
|||||||||||||||||||||
All procedures/treatment requested require |
clinical information (may |
|||||||||||||||||||||||
Health Plan Contact name & phone #: |
|
|
Yes |
|
No |
Authorization Number: |
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
*All sections of this form must be completed.
Pertinent Attachments=Information to support the proposed diagnosis, treatment/procedure; i.e. current clinical findings (progress reports), results
of laboratory testing, imaging studies
**On adverse determinations a reconsideration / expedited appeal may be requested.
* All Sections of this form must be completed.
**On adverse determinations a reconsideration / expedited appeal may be requested.
This referral/authorization is not a guarantee of payment. Payment is contingent upon eligibility, benefits available at the time the service is rendered, contractual terms, limitations, exclusions, and coordination of benefits, and other terms & conditions set forth in the member’s Evidence of Coverage, Certificate of Coverage, or Self Insured Employer’s Plan Documents.
The information contained in this form, including attachments, is privileged and confidential & is only for the use of the individual or entities named on this form. If the reader of this form is not the intended recipient or the employee or the agent responsible to deliver to the intended recipient, the reader is hereby notified that any dissemination, distribution, or copying of this communication is strictly prohibited. If this communication has been received in error, the reader shall notify sender immediately and shall destroy all information received.
Revised 2/24/16
S4590 (02/16)
File Attributes
| Fact Name | Fact Details |
|---|---|
| Form Title | Nevada Universal Prior Authorization and Referral Form |
| Health Plans Covered | Includes Health Plan of Nevada (HPN), Nevada Exchange, Sierra Health and Life, and others. |
| Required Information | All sections must be completed, including patient details, provider information, and treatment requests. |
| Governing Law | Subject to Nevada state laws regarding health insurance and patient confidentiality. |
| Authorization Status | Indicates whether the request is authorized, pended, or denied, along with the reason for denial. |
| Confidentiality Notice | The information is confidential and intended only for the named recipients. Unauthorized use is prohibited. |
Fill out Common Forms
Nevada Medicaid and Nevada Check Up - Find out the role preferred language plays in the Nevada Check Up application process and communication.
For those interested in starting a business in Louisiana, obtaining the Louisiana Articles of Incorporation form from resources such as UsaLawDocs.com is essential, as this document lays the groundwork for establishing your corporation and ensuring adherence to state regulations.
C4 Form Nevada - Agency information, including name and ID, are essential details to be filled in the AD-5 form.